
Let’s start in the
United Kingdom. As I write this the
#nhssm discussion is going on. This was started in 2010 by
Alex Talbott and a
few others and is about how social media might be (and is being used) in
relation to NHS services.
Here on Alex's own blog he discusses some of the practical lessons being learnt by those using social media in healthcare organisation. And from a different angle, in
this storify he describes the concerned response on Twitter of several doctors to the launch of a government campaign to increase awareness
that an unexplained cough may be a symptom of lung cancer. Another GP,
Martin Brunet, has used
his practice blog to explain the background of the campaign to patients and that 'common sense' is needed when interpreting symptoms.
If you are launching a public campaign have a good read at these posts.
How else is social media being used in the UK? Vanguard Health are trying to encourage us to look at the systems in healthcare.
Here Mark Cannon blogs about what he has got out of the use of social media over the past year, although he ends with the reminder that nothing trumps face-to-face relationships. Thinking more broadly than just healthcare,
here @ermintrude2, a social worker who
blogs under a pseudonymn, explains why she thinks
social care also needs social media, and vice versa. Mental health nurse turned manager,
Sarah Amani, tells how s
he started using social media because her professor in an MSc in health care mangement told her it was the best way to stay up to date with research in the field. She describes some of the many benefits blogging and tweeting have had for her.
Let's look at a few posts by
Dr. Mark Newbold, a medically qualified doctor, who is now
Chief Executive of one of the largest NHS trusts in England. Here on his personal blog he gives 1
0 reasons why healthcare CEOs should use Twitter. You will be interested in what happened when his trust decided to have a
Twitter Open Day. Who do you think would engage with a chief executive if he said he would reply to all and sundry? The expectation was that the interaction would mainly be from those using the service, but it wasn't. Instead most tweets came from staff, and this has lead to changes which can be implemented quickly. Who do you think would respond if you ran an activity like this?
But what about the voices of those using the services?
Victoria Betton is doing a PhD on the use of social media in mental health services. She has just posted an interview with
Mark Brown, a mental health campaigner, in 3 posts on her blog. Read all of them, but if you only have time for one read this:
Is the NHS rubbish with social media? If you are fed-up of the rhetoric about the use of social media in healthcare then read this now. Do!
But if you only have time to read one blog post from this entire review then read
this post about patient and disability activist,
Sue Marsh. At the time of writing
this post has 63 comments. It describes an incident that took place last weekend and was watched by thousands on Twitter. After surgery Sue discovered she had been given analgesia which she was allergic too. She tweeted about her distress and this resulted in the columnist for a national newspaper, the Daily Mail, contacting the hospital and asking for a senior nurse to review her case immediately. This happened. Last weekend, the Guardian newspaper, suggested you should
complain on Twitter for an instant response from companies. This blog post describes how patients may also use social media to get help when they are in acute distress within a hospital. This may be something you have not considered before which is why you should read this post.

Of course, we can't leave out the United States, the more usual home of the #hcsm review. Here is
a lovely post by patient turned healthcare advocate, AfternoonNapper, describing what you might get out of becoming an activist: much more than you put in. I think the patient activists I have linked to above would probably agree.
Also from the US, lawyer and HSCM review co-founder.
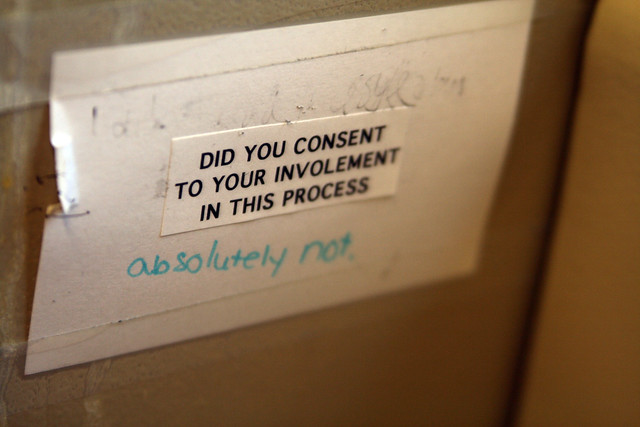
David Harlow, casts
his critical eye over the decision by Facebook to start tracking organ donor status. I have to say that I too was slightly cynical when I read about this. David suggests that monetization as much as medicine might lie behind the decision, but he would like to see Facebook throwing their weight behind a presumed consent law.

And now two posts from the other side of the world, Australia. First up,
Mike Cadogan, an emergency physician, updates the 2009 analysis to
show social media is being used by hospitals in Australia. This is an incredibly detailed post linking to the YouTube, Facebook and Twitter presence of all hospitals there. But Mike is disappointed. Private hospitals are about 10 times as likely to have a social media presence as public hospitals. A bigger question is does this matter?
Tim Senior, a GP with a special interest in Aboriginal health and medical education (who I first met through his
citeulike presence) reminds us that the digital divide is a reality when he writes asking us to "
look in the rear view mirror occasionally". The people who get left behind because they can't or don't access social media, might be those who need healthcare more than any other group.

For a truly global perspective catch
this post by Christopher Purdy about the use of social media around the world to promote sexual health. Here he describes initiatives in Mozambique, Ethiopia, Brazil and Indonesia amongst others.
Closer to (my) home is the upcoming Doctors 2.0 conference in Paris later this year. Joan Justice, HCSMreview co-founder, writes about it
here, whilst organiser Denise Silber i
nterviews a physician and marketing specialist from Italy on the future of mHealth in the EU.

Last but not least, a post from Ireland (I'm from the 1/3 of the way down the Eastern coast, just beside the Mourne mountains).
Dr, Ronan Kavanagh is a rheumatologist
who writes here about why he is a convert to the use of Twitter at conferences. Read and learn about his experiences at the world's biggest rheumatology meeting.
And so concludes this round-up of how social media is being used in healthcare around the world. Tune in next time!
Photo credits :
UK Love by Doug88888
USA flag by FreefotoUK
Ireland by Nasa Goddard Photo and Video
Australia's flag looking like canvas by Chrisser







{kind=link}